




Side Effects of Rural Living: Health Disparities in the Heartland

Thursday November 18th, 2021 is National Rural Health Day. This year the National Organization of State Offices of Rural Health (NOSORH) is specifically highlighting health equity in rural communities. One of the goals of HHRA’s flagship project, The Heartland Study, is to analyze the impact of pesticide exposures on human health, especially on reproductive impacts, healthy pregnancies and children’s development. Our research is already documenting rising levels of herbicide use and exposures across all citizens in the Midwest and rural communities in particular.
Factors impacting the health of rural populations are often underexplored in large scale clinical research projects carried out in large urban centers. According to the U.S. Census Bureau, 97% of land in America is considered rural. Recognition of rural health disparities, and the factors driving them, is an important part of HHRA’s current and future research.
Rural Health Disparity
A whole host of compounding factors have created significant health disparities for rural communities. Rurality is generally classified as any area outside of an urban area. The Census Bureau defines rural as any population, housing, or territory NOT in an urban area. In 2020, there were approximately 57.23 million people living in rural areas in the United States, about 17% of the overall population (Source).
Rural communities are often geographically isolated from the many resources urban and suburban people take for granted. Something as simple as a yearly doctor’s appointment, or finding a healthcare specialist, can be difficult for rural families, due to long distances they may have to travel and limited transportation options. Census data of medical doctors in the US shows that rural areas only have 11 MDs per 10,000 people, compared to 31 per 10,000 in urban/metro areas. In addition, the extent and quality of healthcare services varies greatly across rural regions of the country.
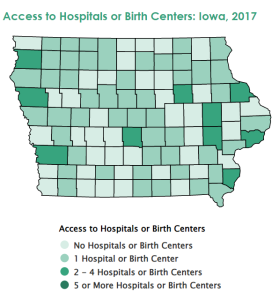
Data from March of Dimes shows how access to hospitals in the Heartland state of Iowa are limited to only a few counties (see map). Many families in rural counties have little or no access to a nearby hospital or birth center. This distance can complicate a person’s ability to get appropriate treatment for serious health problems, especially for rural individuals who don’t have a car, money, or access to transportation.
Lack of access to healthcare resources has a direct impact on the health and quality of life of rural communities. These populations have statistically higher rates of disease and disability, pain, increased mortality, and shorter life expectancies. The top five leading causes of death (heart disease, cancer, unintentional injury, chronic lower respiratory disease, and stroke) are all higher in rural populations compared to urban populations.
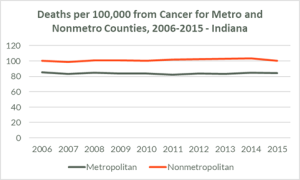
In the Heartland State of Indiana, for example, cancer related deaths are far higher in rural/nonmetro counties than in urban/metro counties (see chart below).
Food insecurity is also higher among rural populations. According to the USDA Economic Research Service report in 2020, 11.6% of rural households are food insecure, compared to 10.5% for the nation as a whole. Child poverty and food insecurity is also higher in rural areas, with 16.1% of rural households with children being food insecure, compared to 14.8% overall.
Inequality and Social Determinants of Health in Rural Populations

Health inequalities are often exacerbated by social determinants of health. Rural Americans are more likely to be low in socioeconomic status or be unemployed, have less post-secondary education, and are less likely to have healthcare coverage by employers or through Medicaid. In addition, rural households have less access to community social programs, foodbanks, and SNAP program benefits.
Social inequities and health disparities go hand in hand. Social determinants of health like income, education, health literacy, environmental health, gender identity, and race/ethnicity all impact an individual’s physical and mental health.
The data backs this up – adults of racial and ethnic populations, living in rural areas, face more health disparities than white adults. A 2017 CDC report showed that Indigenous, Hispanic, and Black individuals in rural areas were more likely to have higher rates of poor health, report multiple chronic conditions, and are at most risk for obesity.
Rural communities may also face more environmental challenges that can impact health. Overall access to safe drinking water, healthy food options, and stable housing is a problem for many rural communities. Hazardous materials often end up in rural areas, contaminating local environments. In farming areas, heavy use of agricultural chemicals can expose both farmers and non-farmers to toxic pesticides in air, water and dust and soil particles. These additional routes of exposure to possibly toxic chemicals are at the crux of HHRA’s scientific research on the impacts of pesticide exposure on reproductive health, pregnancy outcomes and children’s development in the Midwest. By including rurality in our research, we hope to better understand the connections between farming practices, pesticides and other toxins unique to rural areas and public health outcomes.
HHRA is committed to taking account of the impacts of the unique risk factors and unequal access to healthcare services in specific rural areas, as well as gleaning insights from rural-based clinical research. Progress in understanding these factors will help HHRA address how access to food and farming systems impact public health outcomes in the Heartland and beyond.
We are committed to enrolling at least 30% of participants in our flagship project, The Heartland Study, from rural areas. Most clinical research on pregnancy and reproduction takes place in urban research hospitals, and the unique health challenges faced by rural women are often not explored. We want to change that.
This is why HHRA is working to build research capacity in rural hospitals and why we will be recruiting more rural hospitals into The Heartland Study.
We are also hoping to raise adequate funding for 2022 to translate our clinical research documents into other languages. Inclusivity starts with ensuring everyone has a seat at the table, where their voice can be heard.
This #GivingNovember please help us expand our reach to rural families and healthcare providers in the Heartland. You can do so my making a contribution, signing up for the HHRA newsletter and following us on social media.